Oculoplasty is a sub speciality branch of Ophthalmology which deals with structures surrounding the eyeball like orbit (eye socket), eyelids, tear ducts and their reconstructive procedures. It is a highly specialised branch which is capable of giving a major boost to one’s self confidence by enhancing the features of the eyes which are said to be the windows of soul, rectifying deformities and rejuvenating one’s overall appearance and personality.


Oculoplastic surgeons imbibe the finest skills of ophthalmic microsurgery and plastic surgery as they first train as ophthalmologists and later specialise in plastic surgery making them highly skilled surgeons. They have the best knowledge about the eye and its surrounding; as eye surgeons.They are also ready to handle the most delicate of structures. This combination of skills makes the oculoplastic surgeons the best to do plastic surgery around the eye.
Narayana Nethralaya is the first as well as the largest orbit and oculoplasty service in Karnataka. We routinely deal with complex oculoplastic and orbital conditions, which are rarely encountered in general ophthalmology practice. We perform more than 1500 oculoplastic procedures a year. This included 1250 lacrimal surgeries, 250+ ptosis corrections, 500+ orbital diseases in the last 5 years. We believe dealing intensively with rare surgeries and disease helps hone our experience and expertise.
Back in 2004, when oculoplasty as a sub-speciality service was unheard of in Karnataka, Narayana Nethralaya was the first eye hospital to set up an exclusive Oculoplasty department under the able leadership of Dr Roshmi Gupta. Since its inception, our Oculoplasty department has grown leaps and bounds, treating complex cases referred from all over Karnataka and India which makes our Oculoplasty department a tertiary referral care centre. Today we have a team of six trained Oculoplasty surgeons trained at the best centres in India and internationally to keep all your oculoplasty worries at bay.
The Oculoplasty department follows a holistic approach with comprehensive care available under one roof including reconstructive surgery, aesthetic surgery, lacrimal disorders, ocular oncology, anaesthesia care, ocular prosthesis centre, physician care, laboratory facilities including pathology, microbiology and one of its kind GROW lab nurturing research thereby working towards novel treatment techniques.
The Department is well equipped with state of the art laboratory and operating theatre facilities with cutting edge technology combined with a team of highly specialised Oculoplasty surgeons which makes it one of the best Oculoplasty centres in India.
Lid margin malposition is a commonly encountered condition presented to the oculoplasty department.
Blockage of the tear drainage system often leads to troublesome watering and discharge and at times acute infection…
Thyroid dysfunction is a commonly encountered condition which can affect the eyes ranging from bulging of eyes and…
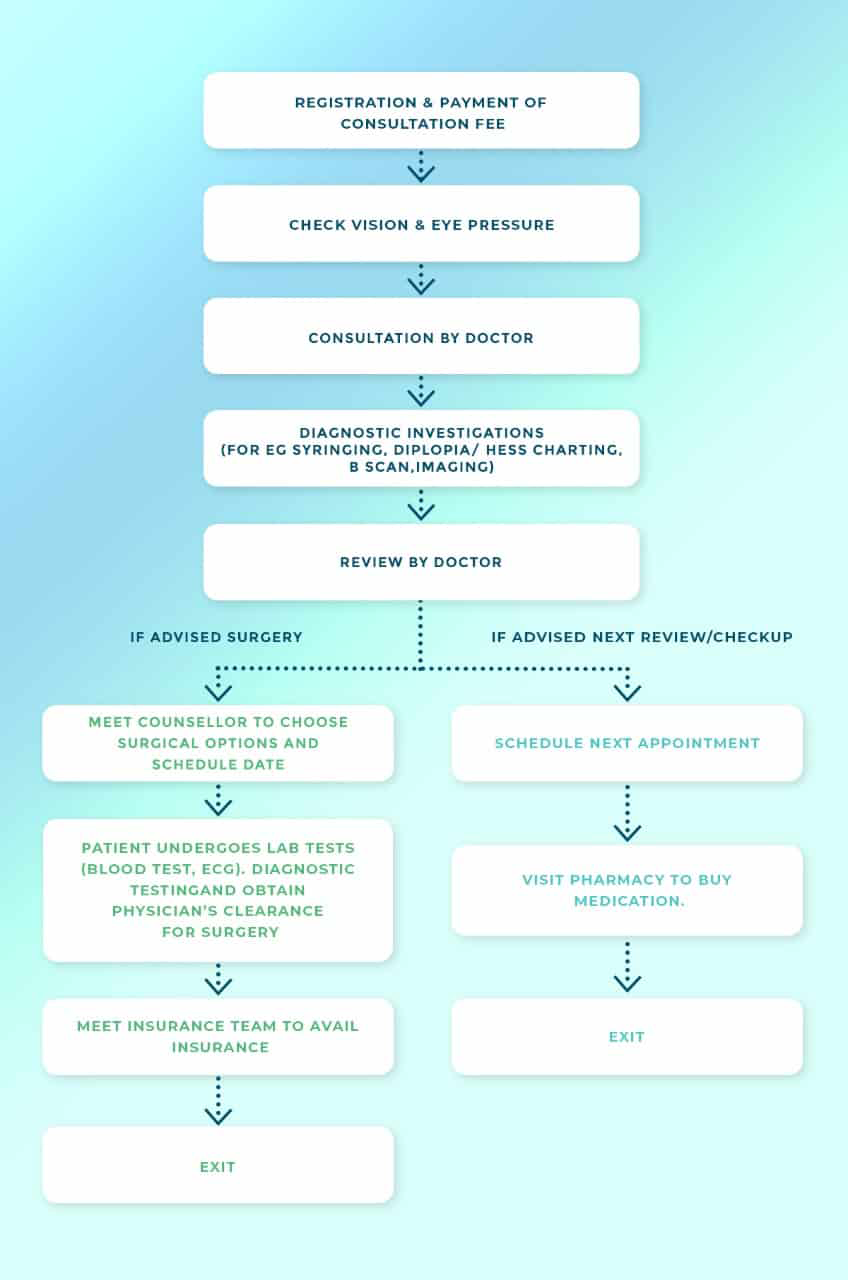
If you have an eyelid margin malposition, troublesome watering or discharge from your eyes, experienced bulging of eyes, experience double vision or reduced vision, notice a lump or swelling growing on your eyelid or a white reflex, it is an appropriate time to schedule an appointment with an ophthalmologist to get your eyes checked in detail. The doctors at Narayana Nethralaya will evaluate the health of your eyes and assess your condition. Your initial consultation will take approximately 2 hours if you do not require cross-consultation and up to 4 hours if you require cross-consultation. During your consultation, our doctors and counsellors will determine the best course of action for your vision needs, go over the risks and benefits of the treatment, and help you choose the best procedure that is suitable for preserving your visual needs. We suggest you bring a family member or friend with you to help you with your decision-making.
A 32 year old gentleman visited Narayana Nethralaya with complaints of prominence of left eye which was gradually progressive over 2 years. Clinical examination revealed proptosis and mass in the superior orbit which was confirmed by CT scan of the orbit and was displacing the muscles around the eyeball . The patient underwent orbitotomy for the removal of the mass and it was removed in toto . The mass was found to be a tumour arising from the sheath around the nerve surrounding the eyeball. The patient is symptom free now with 100 % vision and complete restoration of movements of the eyeball .The surgery was done by an incision along the eyelid crease and hence is almost scarless. The patient is extremely happy and went home satisfied with the services offered to him at Narayana Nethralaya.
A 24 year old young woman visited Narayana Nethralaya with complaints of drooping of right eye upper eyelid from past 4 years . She was extremely unhappy about the asymmetry of her eyes and the patient admitted that it was affecting her matrimonial prospects. After a thorough clinical examination by our Oculoplasty surgeon she was reassured that her condition is due to the disinsertion of the muscle responsible for lifting her eyelid and that a surgery would be sufficient to correct this condition . The patient was apprehensive about the scar . She was reassured that the surgery would be performed by an incision along the eyelid crease and hencethe scar would be hidden along the lid crease & would be scarless for all practical purposes. She underwent ptosis correction surgery and at the end of her 2 week post operative follow up, her eyelids are absolutely symmetrical with respect to the eye opening and contour and she is an extremely happy patient now.
A 55 year old male patient presented to our Oculoplasty Department with complaints of prominence of both eyes with decreased vision in both eyes . He was diagnosed recently with Grave’s disease(a disorder of the thyroid gland which could affect eyes too). Clinical examination revealed decreased vision and colour vision in both eyes, limitation of ocular movements, double vision and compression of the optic nerve. He was started on high dose steroids and since the pressure around the optic nerve was increasing, he was advised orbital decompression surgery which aims at creating space for the enlarged structures around the eyeball. The patient is under regular follow up. The timely intervention prevented irreversible loss of vision and functionality of the muscles around the eyeball. He is an extremely happy patient now with near total restoration of his vision and ocular movements.
At Narayana Nethralaya, we are committed to providing our patients with advanced quality eye care at affordable prices. These eye surgery experiences stand testimony to the excellence in eye care that we offer.

At Narayana Nethralaya, “Quality of Care” and “Patient Safety” is our priority. Concern for our patients’ well being is at the core of what we do, and what drives us. Five units of Narayana Nethralaya are NABH Accredited – the highest national recognition for quality in patient care and safety. Our Oculoplasty team help patients make an informed treatment choice on the type of treatment and surgery that is best suited for their lifestyle. We have an exclusive counseling team to address any doubts or questions that people may have about Oculoplasty treatment options, procedures, preoperative testing and post surgery recovery.